Video-assisted procedure
The aortic valve replacement is a minimally invasive procedure performed by using a mini thoracotomy. With this procedure only a 4-5cm long incision between the ribs is needed, allowing to access the heart without opening the chest. Thanks to the minimally invasive procedure, the duration of the operation is shortened; As a rule, the intervention lasts about two hours. This leads to a shorter post-operative time in the intensive care unit, to fewer blood transfusions, to faster extubating and faster mobilization of the patient. This minimally invasive procedure is an interesting alternative for the TAVI process, which has not been used for so long.
Minimally invasive or «TAVI»
Aortic stenosis is the classic disease of old age and can affect up to 25% of people over 80 years of age. In order to replace the aortic valve that has been stenosed over the years, aortic valve replacement has been performed up to now via median sternotomy. In this procedure, the sternum must be sawed open in the middle to create access to the heart. Sternotomy is also considered the standard access for all other conventional heart operations.
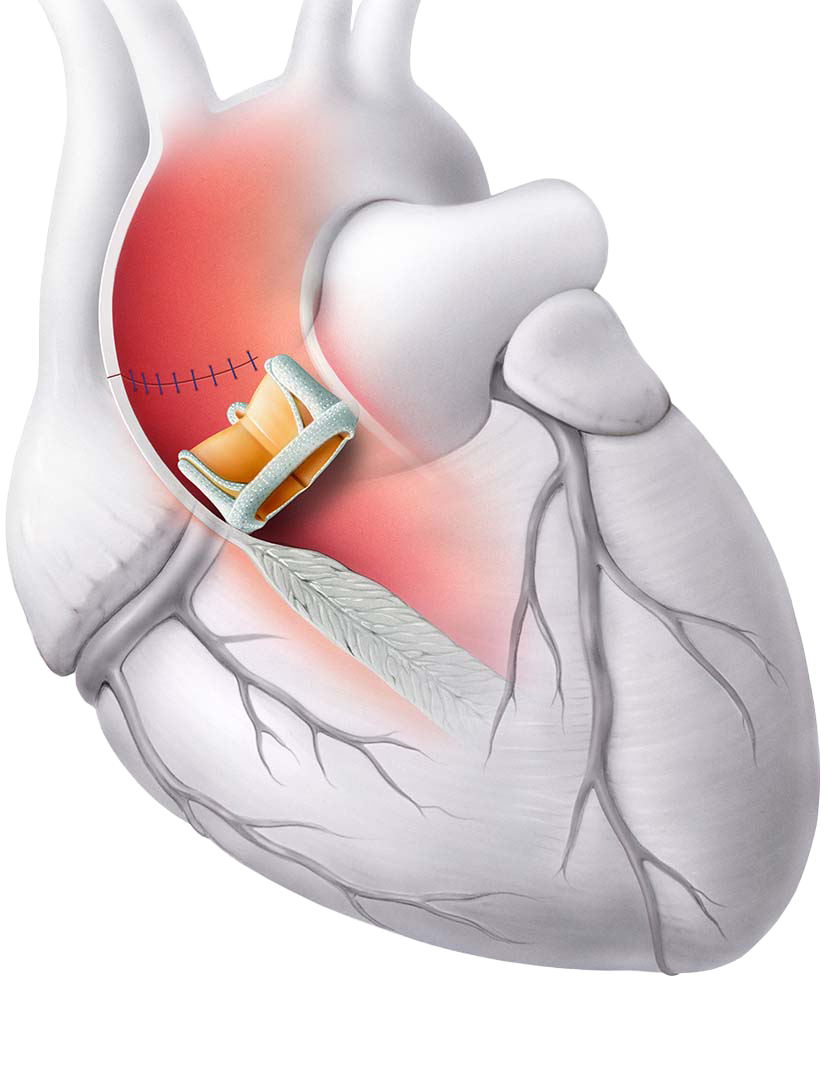
In aortic valve replacement, the aorta is cannulated after the sternotomy and the heart-lung machine is connected to it. The patient is then cooled, the aorta is cross-clamped, and the heart is temporarily immobilized by cardioplegia. During this ischemic period, the calcified aortic valve can be surgically removed, and a new prosthesis can be sewn into the aortic annulus. The procedure is considered the "gold standard" in the treatment of aortic valve stenosis, with excellent long-term results and a low surgical mortality [2].
Due to increasing age and life expectancy, more patients today than ever before undergo aortic valve surgery. This leads to a changed risk profile of patients. In particular, morbidity is related to the invasiveness of the procedure [3].
In order to adapt to these conditions, various innovations have made considerable progress in recent years. In particular, newer surgical techniques have proven to be very helpful [4].
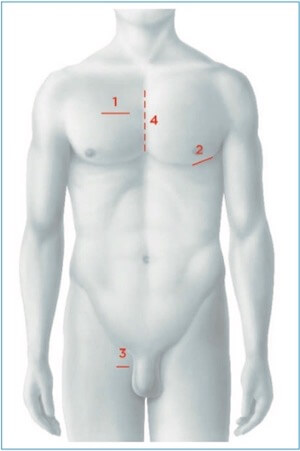
The current trend is towards less invasiveness, which can be achieved by a smaller surgical access, the so-called minimally invasive aortic valve replacement. Here, the thorax is not opened via median sternotomy; access to the aortic valve is created via a mini thoracotomy; the heart-lung machine is connected peripherally (i.e. in the groin) for this access (Fig. 1).
Another strategy to reduce invasiveness is to avoid the heart-lung machine altogether. This is where the "TAVI procedure" is used (TAVI: Transcatheter Aortic Valve Implantation). This is a catheter-based aortic valve replacement. In this procedure a biological prosthesis is implanted either via the groin (transfemoral), via the apex of the heart (transapical) or via a direct transaortic access (Fig. 1).
Which method is chosen depends on the individual circumstances of the patient and must be decided by the Heart team on an interdisciplinary basis before the procedure.
Operation-Method
Conventional Valve Replacement
Aortic valve replacement via median sternotomy has so far been the best way to remove the calcified aortic valve and sew in a new prosthesis. In this procedure, the sternum was sawed open in the middle.
The current trend is towards less invasiveness, the so-called minimally invasive aortic valve replacement, which can be achieved with a smaller surgical access. In this procedure, the thorax is not opened via median sternotomy; access to the aortic valve is created via a mini thoracotomy.
TAVI-Procedure
Another strategy to reduce invasiveness is to avoid the heart-lung machine (HLM) altogether. This is where the TAVI procedure is used (TAVI: Transcatheter Aortic Valve Implantation). This is a catheter-based aortic valve replacement. In this procedure, a biological prosthesis is implanted either via the groin (transfemoral), via the heart tip (transapical) or via a transaortic access (same access as for minimally invasive aortic valve replacement, but without HLM).
Choice of Procedure
Current data regarding the comparison between the two methods is well established. Two-year mortality is lower for the TAVI approach than for conventional aortic valve replacement [6].
If there is an increased EuroSCORE (European system for cardiac operative risk evaluation) or significant comorbidities, the TAVI procedure is the method of choice to eliminate aortic stenosis. In this context, however, the TAVI procedure has never been directly compared to minimally invasive aortic valve replacement, but only to conventional aortic valve replacement with sternotomy.
Patient interview after an aortic valve replacement