
Ablation in stead of life long medications?
The electrophysiological study is a special examination where a catheter is inserted into the heart over the groin. It is usually used for the precise identification of cardiac arrhythmias, for example, in patients with a previous ECG or with unclear symptoms such as palpitations. The advantage of this investigation is that the arrhythmia can be triggered, measured and timed at the time of the procedure. If the arrhythmia is sufficiently confirmed, it can be treated by catheter ablation in the same procedure. Cardiac arrhythmias that make catheter ablation necessary include supraventricular tachycardia or atrial flutter (= variant of supraventricular tachycardia, which manifests itself by a strongly accelerated heart rate, even over a longer period of time).
Atrial fibrillation is a very frequent indication for catheter ablation either as pulmonary vein isolation (rhythm control) or, less frequently, as pacemaker implantation followed by AV node ablation (rate control).
Do you have atrial fibrillation and would like a second opinion or are you not sure whether you need a catheter ablation? One of our specialists will be happy to take the time for a consultation.
What is Rhythm-Control?
Rhythm control is a therapeutic strategy that aims to preserve the natural sinus rhythm. The causal treatment of so-called acquired arrhythmias such as atrial fibrillation begins with adjustment of lifestyle and treating of concomitant diseases such as arterial hypertension and diabetes. Rhythm control can also include taking special medication and a cardioversion. Ablation treatment, is the Gold standard in our view, for rhythm-maintaining therapeutic measures.
Pulmonary Vein Isolation (PVI)
The treatment of atrial fibrillation by isolating the pulmonary veins has existed since the late 1990s. The decisive role for the upswing of this catheter-based therapy was the discovery that extra beats of scattered heart muscle cells in the pulmonary veins close to the heart can trigger atrial fibrillation.
Destroying or isolating these cells is much more effective in preventing recurrence of atrial fibrillation episodes than antiarrhythmic drugs.
The procedure is safe and effective, but requires an experienced team of investigators, perfect peri-procedural organization and sound complication management.
Ablation instead of lifelong medications?
Current studies [1] show that catheter ablation provides better long-term results than lifelong medication. This is especially true if taking the respective medication causes / or can cause problems. Often, patients suffer from taking the medication in a similar way as they suffer from the actual symptoms of the disease, which they are trying to prevent by taking the medication. Medications - but also cardioversions - are only effective to a limited extent in the long term for atrial fibrillation and other arrhythmias.
Thanks to the growing expertise of highly specialised doctors and constantly improving equipment technology (catheters, electrophysiological hardware and software), the electrically misdirected or absent impulses of a few cells can now be precisely measured and localised.
Cryoablation als first-line therapy
With cryoablation, the cause of atrial fibrillation is eliminated using cold. The local application (in the heart) of cold precisely destroys tissue so that they can no longer trigger atrial fibrillation. We use this procedure as an initial therapy for patients with paroxysmal atrial fibrillation or atrial fibrillation that only lasts for a short time (<6 months duration). The procedure usually takes one hour and is performed under deep sedation. If the atrial fibrillation recurs after the first three months (the so-called "blanking period"), a second procedure is indicated.
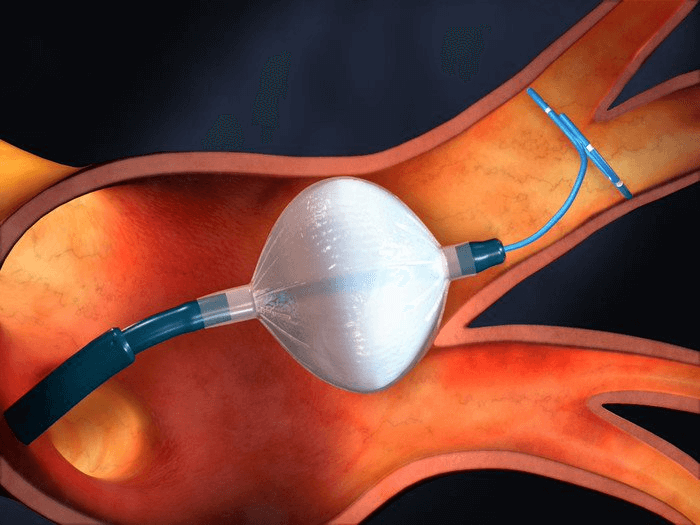
A catheter is advanced into the heart via the groin. There it reaches the left atrium via a transseptal puncture (routine procedure in invasive electrophysiology and cardiology). At this point, the four pulmonary veins are individually cooled down to -60°C for 2 to 4 minutes at their openings by means of the cryoballoon. The "cold burn" produced leads to a circumscribed scarring of the tissue, which means that the disturbing electrical impulse from the pulmonary veins can no longer spread to the heart.
3D-Mapping und RF ablation
With a catheter that is advanced into the heart via the groin under deep sedation, a "3D mapping" - i.e. an electrical map - of the heart's interior can be created "live" (i.e. on the beating heart). On the basis of this precise three-dimensional anatomy and the visualisation of the arrhythmia, the tissue responsible for the arrhythmia can be specifically localised inside the heart and the cardiac arrhythmia can also be terminated in the long term by ablation. The ablation is then done by radio frequency (RF).

Using a catheter that is advanced into the heart via the groin, a "3D mapping" - i.e. an electronic map - of the heart's interior is created "live" (i.e. on the beating heart).
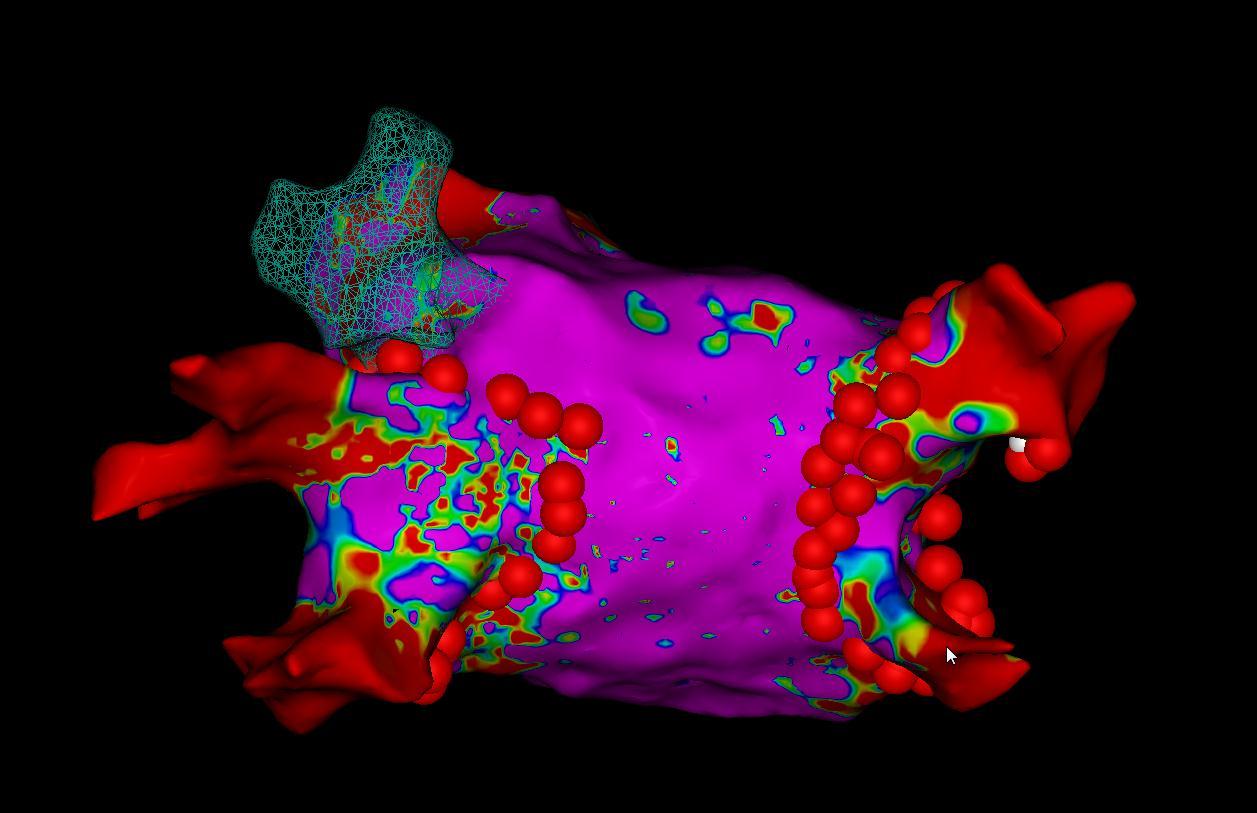
Electroanatomical image of the left atrium. Ablation was performed at the red points (ablated). Circumscribed scars form there, which subsequently prevent the interfering impulses from causing electrical chaos in the atrium. This medical intervention is called pulmonary vein isolation with RF.
Radiofrequency (Heat) oder Freezing (Cold)?
In catheter ablation, the aim is to create a circumscribed scar by obliterating the tissue. This can be used to switch off the arrhythmogenic cells directly or to prevent the abnormal excitation propagation by blocking the conduction. This can be achieved by electric current (RF), cold or laser. No matter which energy source is applied, the tissue is obliterated by the destruction of the cell clusters and a scar is created. The scar is the endpoint of the procedure.
Advantages
The advantage of 3D Mapping and RF Ablation ablation, which is performed under local anaesthesia in twilight sleep - or, if desired, under general anaesthesia - is the possibility to measure and better understand the cardiac current pathways. This is very important in the setting of redo (second or third) procedures.
Who benefits the most?
Most cardiac arrhythmias can currently be treated with catheter ablation, often with significantly better long-term results than with drug therapy. For atrial fibrillation, atrial flutter, paroxysmal supraventricular arrhythmias and some forms of ventricular tachycardia, catheter ablation is the preferred method to permanently stop troublesome episodes. Catheter ablation is performed in a minimally invasive way, so that patients can usually go home after an observation interval of 6 hours. In some situations, the ablation has to be repeated. These include, for example, higher-grade forms of atrial fibrillation. The more advanced the changes in the muscles of the left atrium, the more likely it is that several procedures will be necessary.

The HeartTeam and the patient
The latest guidelines of the European Society of Cardiology from 2020 recommend the cooperation of different specialists (cardiologist, electrophysiologist and cardiac surgeon) in the treatment of atrial fibrillation in order to achieve an optimal outcome for the patient.
This cooperation is summarized under the term "heart team".
Our "Heart-Team" will of course accompany you throughout your entire journey for the duration of your treatment!
References:- Effect of Catheter Ablation vs Antiarrhythmic Drug Therapy on Mortality, Stroke, Bleeding, and Cardiac Arrest Among Patients With Atrial Fibrillation: The CABANA Randomized Clinical Trial – PubMed.gov 2. April 2019